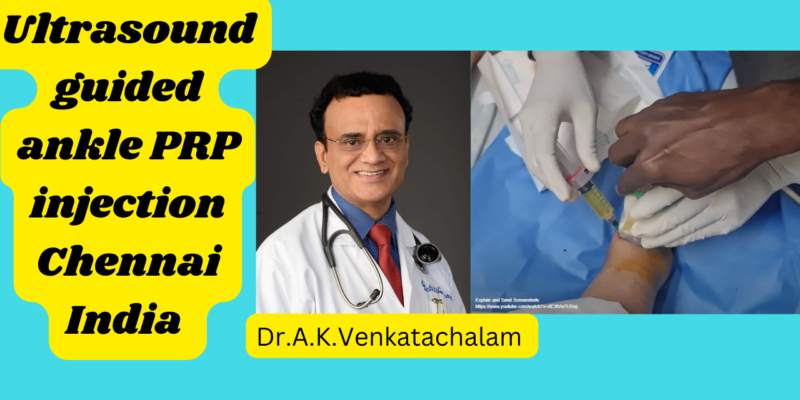
By Dr. A. K. Venkatachalam, Madras Joint Rejuvenation Centre
Introduction
Millions of people receive injections for knee pain every year—PRP, hyaluronic acid, steroids, fat injections, “stem cell” treatments, and more.
Yet many patients tell me the same story:
“Doctor, it worked for a while… and then the pain came back.”
Why do knee injections often fail or give only temporary improvement?
The answer lies in a simple but scientifically supported truth:
See the video here
Osteoarthritis is not a single-layer problem.
It is a multi-tissue, multi-layer disease involving:
-
Synovium – inflammation layer
-
Cartilage – surface integrity layer
-
Subchondral bone – load-bearing & pain layer
If you target only one layer, results will be incomplete.
This is where modern Orthobiologics offer a breakthrough—by matching the right biologic to the right biological target.
⭐ The Knee Is a Biological System — Not a Hinge Joint
Recent research describes the knee as a joint organ.
Synovium, cartilage, meniscus, fat pad, and subchondral bone communicate continuously through biochemical, mechanical, and inflammatory pathways.
This means:
-
Inflammation in the synovium affects cartilage.
-
Weakness or edema in the subchondral bone causes nerve sensitization.
-
Cartilage breakdown exposes bone and triggers more inflammation.
So OA progresses not in isolation, but through interconnected tissues.
⭐ Layer 1: The Synovium (Inflammation Layer)
The synovium is the first tissue to flare in many patients.
MRI studies show that synovitis correlates strongly with knee pain—even more than cartilage loss.
Why inject here?
Because reducing synovial inflammation stabilises the joint environment.
Best biologic for this layer:
-
Leukocyte-poor PRP (LP-PRP)
Evidence shows LP-PRP reduces: -
IL-1β
-
TNF-α
-
Synovial inflammatory markers
This is why I use LP-PRP as the foundation layer in ageing knees.
⭐ Layer 2: Cartilage (Surface Layer)
Cartilage has poor natural repair capacity due to being:
-
Avascular
-
Aneural
-
Low-cellularity
Orthobiologics do not regrow cartilage in advanced osteoarthritis,
but they can improve:
-
Matrix turnover
-
Chondroprotection
-
Joint lubrication
-
Cellular signalling
Best biologic for this layer:
-
Adipose-derived stromal cells (microfat / SVF-rich preparations)
These cells support: -
Matrix maintenance
-
Immunomodulation
-
Cellular cross-talk
In moderate OA, PRP + stromal cells provides stronger and longer symptom relief than PRP alone.
⭐ Layer 3: Subchondral Bone (Load-Bearing Layer)
This is the most overlooked layer, yet it is often the true generator of pain.
Subchondral bone develops:
-
Bone marrow lesions (BMLs)
-
Increased pressure
-
Nerve sensitization
-
Metabolic dysfunction
These changes destabilise the cartilage above.
Why inject here?
Because intraosseous biologics are now shown to:
-
Reduce BMLs
-
Improve load distribution
-
Reduce mechanical pain
-
Support cartilage from below
This is the missing link in many failed treatment attempts.
⭐ Why Injections Fail: The Single-Layer Problem
Most injections target only one of the layers:
| Treatment | Layer Targeted |
|---|---|
| Steroid | Synovium only |
| HA | Lubrication; minor cartilage effect |
| PRP | Primarily synovium |
| Fat (microfat) | Stromal/cellular layer |
| BMAC | Mixed effects but inconsistent |
| “Stem cell” injections | Usually intra-articular only |
If the synovium is treated but the subchondral bone remains diseased, pain returns.
If cartilage signalling improves but synovial inflammation persists, results are weak.
This is why single-injection approaches often fail.
⭐ The 3-Layer Orthobiologic Strategy (My Clinical Framework)
To achieve lasting benefit, each biologic should be chosen according to the target biology:
Layer 1 → Synovium → LP-PRP
Layer 2 → Cartilage → Adipose stromal cells (microfat)
Layer 3 → Subchondral bone → Intraosseous biologics
Not every knee needs all three.
But every knee needs the correct layer addressed.
This biological matching significantly improves outcomes.
⭐ Scientific Support for the 3-Layer Model
Synovium
-
Scanzello CR et al., Bone 2012 — Synovitis drives OA progression
-
Benito et al., Arthritis Rheum 2005 — Pain strongly correlates with synovitis
Cartilage
-
Filardo et al., AJSM 2015 — PRP improves chondrocyte metabolism
-
Buckland J., Nat Rev Rheumatol — MSCs support matrix biology
Subchondral Bone
-
Driban et al., Osteoarthritis Cartilage 2016 — BMLs predict pain & progression
-
Sánchez et al., Int Orthop 2016 — Intraosseous PRP improves BML-related pain
⭐ Who Benefits Most from the 3-Layer Approach?
Ideal candidates include:
-
Men and women 45+
-
With chronic knee pain
-
Early-to-moderate osteoarthritis
-
MRI showing synovitis or BMLs
-
Recurrent pain after PRP or HA
This approach is especially useful in post-menopausal women and metabolically inflamed knees.
⭐ Conclusion
Knee osteoarthritis is not a one-layer problem.
It is a multi-system joint disease, and orthobiologic treatments must be matched to each biological layer:
-
LP-PRP → inflammation
-
Stromal cells → cartilage & signalling
-
Intraosseous biologics → subchondral bone
This 3-Layer model is scientifically grounded, clinically logical, and highly effective for personalized knee preservation.
Q1. Why do knee injections stop working after a few months?
Because they usually treat only one layer (synovium or cartilage) while OA is a multi-layer disease involving synovium, cartilage, and subchondral bone.
Q2. What is the 3-layer orthobiologic approach?
A modern strategy targeting synovial inflammation, cartilage signalling, and subchondral bone remodeling with different biologics.
Q3. Is PRP enough for knee arthritis?
In early OA—sometimes. In moderate OA—usually not. LP-PRP is Layer 1 only.
Q4. Do adipose stromal cells grow new cartilage?
No. They improve signalling, reduce inflammation, and stabilise cartilage microenvironment.
Q5. What is intraosseous PRP?
A targeted biologic injection into the subchondral bone to reduce bone marrow lesions and mechanical pain.
Q6. Who benefits most from this approach?
Patients above 40, especially with synovitis, BMLs, or metabolic knee inflammation.